It is simply absurd to claim that any one human being today hatched their idea out of thin air. There is a chain of education and events to a moment in time that is supported by the generations of humanity previous. There is an unspoken etiquette in the field of science that you cite the person you got the idea from if it isn't totally original. There can be some heated disagreements as to chronology such as the whole DNA structure thing. To all that human misery, I say: "whatever..." Such mundane trifles are the stuff of little men, and little women in the intellectual sense, not the physical sense.
I went for 20 years or so before running into the idea of Vitamin C as a preventive cure for atherosclerosis. At the time it had to do with preventing cholesterol oxidation and blowing bile cholesterol out your rear end. There wasn't a whole lot of sophistry behind what I knew other than the fact that the last time I measured my LDL, it was below normal. Youth had a lot to do with it, maybe even youthful malnutrition, but I knew that the bogus prescription medicines story couldn't be true. At the time, all doctors knew that oat, apple, vegetable, grain, and fruit fibers were enough to sequester colonic cholesterol enough to lower LDL. So why bother with all this toxic fibrate crap and all the rest? Statins are a fungal poison originally designed with cancer in mind. In fact, the first statins are so toxic, they cause cell cycle arrest by poisoning the mevalonate pathway, the one doctors poison now with statins! Does it make sense? Of course it doesn't. Neither did doctors recommending tobacco smoking on national TV and ashing out on the floor of hospitals as they treated their heart patients.
Eventually, I ran across Matthias Rath/Linus Pauling's ideas which were logically satisfying rather than totally illogical like the chemotherapy concept - "Kill the tumor before the chemicals kill you." OF COURSE Dr. Rath and Dr. Pauling are whom I got the idea from to design the animal. Any resistance offered to me at various times by other people are from a simple but somewhat pitiful reason - human jealousy. To this I just remark - it WASN'T these jealous detractors who risked everything to try it. They did not, and they would not now have tried it either. Certainly, had this not all matched up as a theory, I would have been ruined. It's my whole credibility at stake too.
The Ice Age – Cardiovascular Disease Connection
"These effects are achieved by nutritional supplements reversing impaired
blood flow to the heart muscle as well as improving metabolism of
millions of heart cells. The most important among these nutrients are
vitamin C, vitamin E, niacin, lysine, proline, coenzyme Q10, carnitine
as well as certain minerals. Particular emphasis in the book is given to
my earlier discoveries of the therapeutic effect of ascorbate, lysine
and related compounds in neutralizing the risk from lipoproten(a).5
Moreover, a new therapeutic mechanism is described by which lysine and
proline, together with other essential nutrients, decrease the
"atherosclerotic tumor" in the vascular wall caused by smooth muscle
cells." //
Okay, sure. Foam cells - don't forget about them. They are not as irritating as they appear because....Foam cells do not happen in the ears, the nose, the knees, the veins; they simply never occur there. We know now that foam cells locate at the hemodynamically prone areas just where the atherosclerotic SMC tumor may arise too. They can overlap. Lp(a) is always found in a plaque, whatever kind it is, if there is Lp(a) in the blood. I have yet to see one without Lp(a) in it. What are they? Intra-arterial fat cells. Just as specialized adipose can expand and get rid of lipids, so can foam cell lesions expand, shrink, and vanish. The fact that foam cells are present in arteries of people of all ages indicates their normal function beyond their pathological one, which does exist. The debate about the immune system in the artery in health and atherosclerosis is too long to address in one page but do not contradict the findings of Matthias Rath. One group says that macrophages do not respond to vitamin C...in an ApoE KO system. The ApoE KO mouse is like a one-way train. It may leave the home station, but it cannot return. No such thing in people except in cases of sporadic familial hereditary mutations. HDL is the vehicle to which ApoE hands off its cargo among other ways, but LDL can also assume the function of reverse transport to the liver too. HDL can also assume the function of forward cargo carrier too, and does in wild mice! So it is very much not so simple as it is made to appear.
What is straightforward is that a lack of Vitamin C creates the damage that triggers the repair in an artery. However the repair occurs, if it keeps going for decades without stop, it is like building a pile of stuff over the same spot over and over which is exactly what an advanced plaque looks like - an old tree with many rings of stuff. It may be rings of the same stuff or a variegated mixed composition plaque. The lipid core plaque, the obsession of many human cardiologist/statin salesmen for its cholesterol composition, the foam cell lesion the obsession for its chemokine triggered quality thereby justifying ox-LDL, the fibrous lesion obsessed on for being evocative of simplistic old school "arteriosclerosis," and "arterial stiffening" which is true but hardly so simple, calcium the love of the fast CT people and EDTA chelator people, the smooth muscle tumor may or may not be there, or they may all be piled one on top of one another in one portmanteau lump. All these various events are goaded along by a lack of ascorbate ion above a critical efficacy threshold. If 500mg were all anybody needed in a day, why would we bother? We would just close shop and declare, "That's it everybody, all you need is this mediocre fruit juice gamish and that is the end of the story." Unfortunately, the drought of vitamin C is caused by a genetic defect. Genetic defects require the gene product to be rescued in the amount that was once there, not less.
"My earlier publications in the Journal of Orthomolecular Medicine
triggered repeated interest in the history of these discoveries. Thus, a
brief personal chronology may be in order: In 1987, after having
discovered the lipoprotein(a)-vitamin C connection I recommended vitamin
C supplementation to an individual with high lipoprotein(a) levels.
This marks the first therapeutic attempt to lower elevated blood
concentrations of this risk factor by using vitamin C.8,9 During my
research project at Hamburg University I used L-lysine and synthetic
lysine analogs to isolate lipoprotein(a) from blood and from arterial
walls. This suggested the therapeutic use of lysine and synthetic lysine
analogs5, a therapeutic technology for which I recieved patents in the
meantime.. In early 1990, after the prominent role of lipoprotein(a) in
human atherosclerosis was established 10, I came to the United States to
work on the physiologic role of lipoprotein(a) as well as to pursue my
earlier therapeutic discoveries."
So there you have it. The crossing of the animal did not occur to anyone but me, but the application of vitamin C, L-Lysine, and nutrients to prevent atherosclerosis was not my idea but a Dr. Matthias Rath and a Dr. Linus Pauling. There were others afterwards who helped the stage for the ultimate test of the concept which is incredibly important, but saying they were responsible for the idea is like saying I am the discoverer of the DNA structure. (I am not.) I am also not responsible for many amazing ideas in this world, but I don't go insane and try to become responsible for each and every great idea in the world. There would be something wrong with my brain if I were to do that. I hope that all the great scientists of this world achieve their wish of personal discovery and get to see it...before the day they die.
Friday, December 18, 2015
Friday, November 27, 2015
High shear stress. wait wait wait, no. Low shear stress. Wait wait. Low then high shear stress. Oh, okay high shear stress too.
The problem is that you don't have high shear stress WITHOUT high tensile strain, all while disregarding oscillatory tensile strain, pulsatile acceleration between peak systole and diastole, as well as vortice formation.
In my own opinion after carefully digesting all viewpoints, it seems that tensile stress and vortice formation are the most important damaging forces upon an artery. Shear stress is most contradictory if you disregard vortical turbulence/stagnation, and once again, tensile strain.
Shear stress is basically "drag." Like a hand in the wind palm forward, the drag on it is higher than when the hand is held parallel to the wind, creating less drag. How high drag is better for the artery than low drag is explained by the high drag drawing the endothelium tight, like a comb over a dogs' fur in a straight, undeviating stroke. Low drag is supposedly bad for an artery because it doesn't pull the cells tight. To me that doesn't make a lot of sense, but when pulsatile flow (a slight backwards flow on diastole with a majority forward flow on systole) is taken account, that makes sense. Also, vortical formation, is important, but these things are never mentioned in one sentence, causing major confusion. It is not that hard to understand together, it makes it more confusing and ambiguous not to talk about all these things at once. Low shear stress + pulsatile flow caused by a local pressure differential + vortices (tornados of the blood) cause the endothelium to become dissheveled. Like taking your hand and making random circles in your pet's fur, this will cause the once linearly oriented cells to become haphazardly arranged rather than in the direction of the laminar flow.
It is counterintuitive. LOW SHEAR STRESS causes atherosclerosis not high shear stress. Studies in coronary arteries show a precise opposition between high shear areas free of plaque and the low shear area laden with plaque. The problem most have is to confuse shear stress with tensile stress (combined radial, circumferential, longitudinal). Like the thumb and the toe, they are absolutely different things. But more confusing, when there is a big plaque, there is high shear stress in the throat it makes with lumenal occlusion. Then, high shear stress may rip open the plaque, causing thrombosis and downstream ischemia. All the while, tensile stress is proportional to shear stress, and higher tensile stress causes more load on the force bearing elements of the arterial ECM, which invariably only causes one thing: wear and tear (literally).
With venous systolic pressure up to ten times lower than arterial systolic pressure, it is not difficult to understand why arteries always endure more tensile strain. Whatever the shear stress condition, tensile strain in the artery is always higher than in a vein, partially explaining why only thrombosis is found in veins but no plaque. It is interesting to note that a vein placed in the coronary bed for bypass does then suffer plaque stenosis when it never did before. What is the sudden difference? Systolic pressure and tensile strain is much higher in the arterial bed.
Yet there are instances when high shear stress contributes to arterial damage, such as a biscupid aortic valve.
 You'll see above, that the high shear stress area (which is invariably a zone of high tensile strain) coincides perfectly with proximal aortic dissection, the Stanford Type A, Debakey Type II dissection, as well as a frequent site of aortic root (not sinus) plaques.
You'll see above, that the high shear stress area (which is invariably a zone of high tensile strain) coincides perfectly with proximal aortic dissection, the Stanford Type A, Debakey Type II dissection, as well as a frequent site of aortic root (not sinus) plaques.
Valve-Related Hemodynamics Mediate Human Bicuspid Aortopathy
In my own opinion after carefully digesting all viewpoints, it seems that tensile stress and vortice formation are the most important damaging forces upon an artery. Shear stress is most contradictory if you disregard vortical turbulence/stagnation, and once again, tensile strain.
Shear stress is basically "drag." Like a hand in the wind palm forward, the drag on it is higher than when the hand is held parallel to the wind, creating less drag. How high drag is better for the artery than low drag is explained by the high drag drawing the endothelium tight, like a comb over a dogs' fur in a straight, undeviating stroke. Low drag is supposedly bad for an artery because it doesn't pull the cells tight. To me that doesn't make a lot of sense, but when pulsatile flow (a slight backwards flow on diastole with a majority forward flow on systole) is taken account, that makes sense. Also, vortical formation, is important, but these things are never mentioned in one sentence, causing major confusion. It is not that hard to understand together, it makes it more confusing and ambiguous not to talk about all these things at once. Low shear stress + pulsatile flow caused by a local pressure differential + vortices (tornados of the blood) cause the endothelium to become dissheveled. Like taking your hand and making random circles in your pet's fur, this will cause the once linearly oriented cells to become haphazardly arranged rather than in the direction of the laminar flow.
It is counterintuitive. LOW SHEAR STRESS causes atherosclerosis not high shear stress. Studies in coronary arteries show a precise opposition between high shear areas free of plaque and the low shear area laden with plaque. The problem most have is to confuse shear stress with tensile stress (combined radial, circumferential, longitudinal). Like the thumb and the toe, they are absolutely different things. But more confusing, when there is a big plaque, there is high shear stress in the throat it makes with lumenal occlusion. Then, high shear stress may rip open the plaque, causing thrombosis and downstream ischemia. All the while, tensile stress is proportional to shear stress, and higher tensile stress causes more load on the force bearing elements of the arterial ECM, which invariably only causes one thing: wear and tear (literally).
With venous systolic pressure up to ten times lower than arterial systolic pressure, it is not difficult to understand why arteries always endure more tensile strain. Whatever the shear stress condition, tensile strain in the artery is always higher than in a vein, partially explaining why only thrombosis is found in veins but no plaque. It is interesting to note that a vein placed in the coronary bed for bypass does then suffer plaque stenosis when it never did before. What is the sudden difference? Systolic pressure and tensile strain is much higher in the arterial bed.
Yet there are instances when high shear stress contributes to arterial damage, such as a biscupid aortic valve.

Valve-Related Hemodynamics Mediate Human Bicuspid Aortopathy
Saturday, November 21, 2015
Superb Blog of Blog: "Ancient Transporters: HDL and LDL Lipoproteins Carry Precious Cargo "
This is a scientific island of common sense worth visiting. Extremely insightful and ties together things far apart for an understanding with "range."
http://drbganimalpharm.blogspot.com/2013/03/ancient-transporters-hdl-and-ldl.html
http://drbganimalpharm.blogspot.com/2013/03/ancient-transporters-hdl-and-ldl.html
Forced Reading Versus Searched Reading
Some people will spend hundreds of thousands of dollars on forced exposure to an idea. You have no choice but to look at it, imprinting an idea in your mind, whether you agree to it or disagree to it. That is one approach. There may be some big proponents you win this way, as well as big opponents.
On the other hand, the totally free, no money involved Google Blogs only attract people who resonate with your idea. In essence, you automatically generate 100% support bases by not spending any money, not trying (at all) to attract anyone. Agree? Stay. Disagree? Okay, you didn't lose anything so don't stick around. Especially don't stick around and disagree. I spent $0 on gaining a philosophical support base but that is not the correct or appropriate way to look at things. More accurately, like minded people eventually resonate toward one another try or not to keep them away from one another.
Or you can try to force the same poles of two magnets against one another, causing only repulsion, to use a metaphor.
In a way, simply typing this forces (somebody) to read this. I didn't spend anything other than a few minutes and a few electrons doing this. It only takes one power broker or gatekeeper to agree with you (or disagree with you as it may be) to change the intellectual terrain on which you are received. By voicing your thoughts (for free, not forcing people to read with hundreds of thousands of dollars), you activate this possibility. If you don't, what can happen other than nothing changing...
In this regard, I see that there are classically trained and intelligent scientists who are separating the bogus chaff of sales pitches from the drug industry from what is real, and too bad for the drug salesmen, oftentimes the real solution is not a big money maker. Good for you, you reader! Congratulations on finding my shared knowledge, you will not regret it but rather free yourself from the exponential chain of bullshit that will cost you lots money, time, and pain.
If you don't agree, just go away. It is like the Flinstonian obsolete creeky old institution The Freemasons, feebly trying to make a comeback in places like Orange County, CA believe it or not. The Freemasons don't go out like Jehovah's Witnesses trying to recruit people let alone retain them. Come and stay, or come and go, or don't come, or stay and go, whatever. It is totally up to you. I simply go to a Roman Catholic church and pay my dues in work or support, it is much easier and cheaper. Humans think they can pay their way into some unknown or worse confuse science with religion which even a priest would advise against. But as Einstein said, "God does not play dice with the universe." No, it is intentional. If you are so obtuse not to see these workings, it is no use to force this understanding. A person changes his or her own mind or heart, there is no other path in intellectual concession. A person celebrates in "changing someone else's mind." Ridiculous. Nobody changes anyone's mind, they change their own.
On the other hand, the totally free, no money involved Google Blogs only attract people who resonate with your idea. In essence, you automatically generate 100% support bases by not spending any money, not trying (at all) to attract anyone. Agree? Stay. Disagree? Okay, you didn't lose anything so don't stick around. Especially don't stick around and disagree. I spent $0 on gaining a philosophical support base but that is not the correct or appropriate way to look at things. More accurately, like minded people eventually resonate toward one another try or not to keep them away from one another.
Or you can try to force the same poles of two magnets against one another, causing only repulsion, to use a metaphor.
In a way, simply typing this forces (somebody) to read this. I didn't spend anything other than a few minutes and a few electrons doing this. It only takes one power broker or gatekeeper to agree with you (or disagree with you as it may be) to change the intellectual terrain on which you are received. By voicing your thoughts (for free, not forcing people to read with hundreds of thousands of dollars), you activate this possibility. If you don't, what can happen other than nothing changing...
In this regard, I see that there are classically trained and intelligent scientists who are separating the bogus chaff of sales pitches from the drug industry from what is real, and too bad for the drug salesmen, oftentimes the real solution is not a big money maker. Good for you, you reader! Congratulations on finding my shared knowledge, you will not regret it but rather free yourself from the exponential chain of bullshit that will cost you lots money, time, and pain.
If you don't agree, just go away. It is like the Flinstonian obsolete creeky old institution The Freemasons, feebly trying to make a comeback in places like Orange County, CA believe it or not. The Freemasons don't go out like Jehovah's Witnesses trying to recruit people let alone retain them. Come and stay, or come and go, or don't come, or stay and go, whatever. It is totally up to you. I simply go to a Roman Catholic church and pay my dues in work or support, it is much easier and cheaper. Humans think they can pay their way into some unknown or worse confuse science with religion which even a priest would advise against. But as Einstein said, "God does not play dice with the universe." No, it is intentional. If you are so obtuse not to see these workings, it is no use to force this understanding. A person changes his or her own mind or heart, there is no other path in intellectual concession. A person celebrates in "changing someone else's mind." Ridiculous. Nobody changes anyone's mind, they change their own.
Bathe your insides with green plant juice.
Why would you do that???
TNF-alpha shreds your arteries and causes plaque to start forming
Chlorophyll prevents TNF-a from doing its business to you.
Therefore, green plant juice may prevent atherosclerosis.
TNF-alpha shreds your arteries and causes plaque to start forming
Chlorophyll prevents TNF-a from doing its business to you.
Therefore, green plant juice may prevent atherosclerosis.
Sunday, November 15, 2015
Negligence. Obfuscation. Perdition. Eloquence. = NOPE
As a wise man once said, there is no long term benefit to mediocrity. If it brings you to a show, helps make money in the short term, but is totally mundane and forgettable, all that will happen is that you as a scientist will have wasted your time, maybe even your entire life into your 60's, chasing after chimeras. ghosts. illusions. nothing. By that age, it is way too late to "start fresh." At best, you will be a walking irrelevent obsolescence, rotting by the day to the grave, comfortably but kindly unknown to anybody.
What is worse is when someone intentionally ignores uncomfortable or contrary evidence. Not refutes, but ignores. Refuses to even read and acknowledge. Then obfuscation, which some quackademians are experts at, leaves a smoke screen so thick that some people give up trying to understand them, leaving them to go their merry but incorrect way. Of course, if these people are wrong, fallacious, or inaccurate, it is simply a matter of time before the world makes fools of them, flying them like a flag for others to ridicule. In this way, perdition is the fire under every good scientist's ass that should make sure they are honest. I feel the heat everyday and this does make sure that I never even entertain the thought of "fudge factor" or some white lie. Even the most eloquent liar eventually gets turned up as a ridiculous fraud which is why I would never attempt such a moronic thing. Such charlatans get written up in history to be ridiculed FOREVER.
Yet others do, for short term benefits or whatever. Not me. N.O.P.E. If someone tries to stuff words in my mouth, I will swiftly and sternly correct their dishonesty in a very public way. Have a question about my work? Ask me directly, not some crazy second-hand competitor. - John C. Cha
Don't let the clowns of NOPE tell you what I think as they do not know what I think.
What is worse is when someone intentionally ignores uncomfortable or contrary evidence. Not refutes, but ignores. Refuses to even read and acknowledge. Then obfuscation, which some quackademians are experts at, leaves a smoke screen so thick that some people give up trying to understand them, leaving them to go their merry but incorrect way. Of course, if these people are wrong, fallacious, or inaccurate, it is simply a matter of time before the world makes fools of them, flying them like a flag for others to ridicule. In this way, perdition is the fire under every good scientist's ass that should make sure they are honest. I feel the heat everyday and this does make sure that I never even entertain the thought of "fudge factor" or some white lie. Even the most eloquent liar eventually gets turned up as a ridiculous fraud which is why I would never attempt such a moronic thing. Such charlatans get written up in history to be ridiculed FOREVER.
Yet others do, for short term benefits or whatever. Not me. N.O.P.E. If someone tries to stuff words in my mouth, I will swiftly and sternly correct their dishonesty in a very public way. Have a question about my work? Ask me directly, not some crazy second-hand competitor. - John C. Cha
Don't let the clowns of NOPE tell you what I think as they do not know what I think.
Sunday, November 1, 2015
Do not take Vitamin D for flu prevention?!? A world gone mad and dishonest.
Epidemic influenza and vitamin D
With a clear link to Vitamin D deficiency and influenza having been established by the most credible doctors and scientists to have existed, we have the same message being thrown at us: Get flu shots. Just in time for "flu season" which really coincides with: temperature decrease, aridity of nasopharyngeal mucous membranes, and Vitamin D deficiency (not a weakened flu virus injection deficiency).
As in literally, weakened whole flu virus and sometimes some bonus mercury if the needles were bundled in packs rather than individually. A lot of dummies think that the flu shot is a special medicine, antibody, or nanobot going around inside you plucking off the influenza virus. The flu vaccine IS the flu virus. As these rigorous and conventionally trained doctors and scientists documented, Vitamin D deficiency caused this flu virus jab to spring into action and cause flu symptoms. The symptoms were minimal to none with lots of Vitamin D.
Yet, because Big Pharma thinks we are morons and only potential consumers, they will try to persuade us to part with our money in any way imaginable. At the top of these industries, literally the only thing that matters is money. Murder is just fine if it means preserving a financial domain. It is not a second thought. If that is okay, then the other things seem like saintly occupations by comparison. What what it be to them to lie to you about efficacy, side effects, or reason of being (money)? As all (ethical) global intelligence agencies do, they follow the money to end at the real source of crime.
With a clear link to Vitamin D deficiency and influenza having been established by the most credible doctors and scientists to have existed, we have the same message being thrown at us: Get flu shots. Just in time for "flu season" which really coincides with: temperature decrease, aridity of nasopharyngeal mucous membranes, and Vitamin D deficiency (not a weakened flu virus injection deficiency).
As in literally, weakened whole flu virus and sometimes some bonus mercury if the needles were bundled in packs rather than individually. A lot of dummies think that the flu shot is a special medicine, antibody, or nanobot going around inside you plucking off the influenza virus. The flu vaccine IS the flu virus. As these rigorous and conventionally trained doctors and scientists documented, Vitamin D deficiency caused this flu virus jab to spring into action and cause flu symptoms. The symptoms were minimal to none with lots of Vitamin D.
Yet, because Big Pharma thinks we are morons and only potential consumers, they will try to persuade us to part with our money in any way imaginable. At the top of these industries, literally the only thing that matters is money. Murder is just fine if it means preserving a financial domain. It is not a second thought. If that is okay, then the other things seem like saintly occupations by comparison. What what it be to them to lie to you about efficacy, side effects, or reason of being (money)? As all (ethical) global intelligence agencies do, they follow the money to end at the real source of crime.
Cholesterol does not cause atherosclerosis. Oxidized cholesterol byproducts do.
Here are a few things to keep in mind: 1) Cholesterol is not soluble in water or blood. A derivative of cholesterol that is soluble in blood or water is not cholesterol. 2) The only way cholesterol is moved around either in the blood or as an adduct is by the action of adding a hydrophilic protein or converting free cholesterol enzymatically to a soluble form. 3) The only way cholesterol gets to an artery wall is through a lipoprotein or the soluble form made first by a cell's action upon ingested cholesterol. 4) It has already been proven that native LDL is harmless to endothelial layers even in very high concentrations of the particle and that the oxLDL particle is the one that causes havoc to the endothelial layer.
That being said, even in the most severely diseased coronary artery disease (CAD) patient with acute coronary syndrome (ACS) presenting as angina, respiratory problems, and/or MI, the level of oxLDL is 4-5mg/dL maximally. Normally, they are half this value to none. This value of 4-5 doesn't occur until after the coronary artery disease, so how could it be that oxLDL caused the CAD? Temporally, and logically, oxLDL could not have caused CAD if it was absent beforehand.
There is no question that toxic adducts of cholesterol DO cause arteriosclerosis and the consequence is atherosclerosis. Is it an inevitable event that cholesterol becomes 25-hydroxycholesterol and cholestane-3beta, 5alpha, 6beta-triol, the culprits of endothelial aggravation? No.
It is not cholesterol, it is OXIDATION that causes these culprit oxidized cholesterol molecules to arise and cause harm. By having administered pure non-oxidized cholesterol to the artery cells with no harm, scientists made sure of the fact as early as 1976. Extending the first post, here are younger studies confirming the first.
Effect of auto-oxidation products from cholesterol on aortic smooth muscle cells: an in vitro study.
Cytotoxicity of oxidation derivatives of cholesterol on cultured aortic smooth muscle cells and their effect on cholesterol biosynthesis.
Ironically, the hydroxycholesterol and other oxygen adducts shut off cellular cholesterol synthesis, making the matter worse as your cells, especially the fastest dividing ones, make it for a mission critical reason. As the repeat, "Purified cholesterol showed no cytotoxic effect and minimal inhibition of cholesterol biosynthesis"
Inhibitory effect of cholesterol oxides on low density lipoprotein receptor gene expression.
Again, after two decades, the groups repeat that ". Pure cholesterol showed only minimal inhibition."
The question of importance is how much of the toxic oxygenated cholesterol is there in food? Who would know for something boiling around in hot oil and open air for weeks? My guess is a significant amount of cholesterol has turned to ox-cholesterol and probably stuff like that should be avoided. Minimally cooked foods, or fresh foods would have a minimum of this toxic cholesterol derivative. So indeed, the way meat is cooked may be a significant way to introduce these cholesterol-oxygen problem compounds in the blood, and these are indeed soluble.
However, like most everything, there is a reason for this artery aggravating 25-hydroxycholesterol (immune response against viruses) to exist:
Armand-Frappier Outstanding Student Award--The emerging role of 25-hydroxycholesterol in innate immunity.
25-Hydroxycholesterols in innate and adaptive immunity.
There is an enzyme that responds to interferon by hydroxylating cholesterol. 25HC is antiviral.
Given that your blood levels of ApoB bound cholesterol are from your liver and not from a vat of oil boiling around for weeks, it would not cause any arterial injury. This is dependent on antioxidant functions preventing oxidation. These are enzymatic, such as PON and glutathione, and enteral/parenteral such as Vitamin C, E, and A.
That being said, even in the most severely diseased coronary artery disease (CAD) patient with acute coronary syndrome (ACS) presenting as angina, respiratory problems, and/or MI, the level of oxLDL is 4-5mg/dL maximally. Normally, they are half this value to none. This value of 4-5 doesn't occur until after the coronary artery disease, so how could it be that oxLDL caused the CAD? Temporally, and logically, oxLDL could not have caused CAD if it was absent beforehand.
There is no question that toxic adducts of cholesterol DO cause arteriosclerosis and the consequence is atherosclerosis. Is it an inevitable event that cholesterol becomes 25-hydroxycholesterol and cholestane-3beta, 5alpha, 6beta-triol, the culprits of endothelial aggravation? No.
It is not cholesterol, it is OXIDATION that causes these culprit oxidized cholesterol molecules to arise and cause harm. By having administered pure non-oxidized cholesterol to the artery cells with no harm, scientists made sure of the fact as early as 1976. Extending the first post, here are younger studies confirming the first.
Effect of auto-oxidation products from cholesterol on aortic smooth muscle cells: an in vitro study.
Cytotoxicity of oxidation derivatives of cholesterol on cultured aortic smooth muscle cells and their effect on cholesterol biosynthesis.
Ironically, the hydroxycholesterol and other oxygen adducts shut off cellular cholesterol synthesis, making the matter worse as your cells, especially the fastest dividing ones, make it for a mission critical reason. As the repeat, "Purified cholesterol showed no cytotoxic effect and minimal inhibition of cholesterol biosynthesis"
Inhibitory effect of cholesterol oxides on low density lipoprotein receptor gene expression.
Again, after two decades, the groups repeat that ". Pure cholesterol showed only minimal inhibition."
The question of importance is how much of the toxic oxygenated cholesterol is there in food? Who would know for something boiling around in hot oil and open air for weeks? My guess is a significant amount of cholesterol has turned to ox-cholesterol and probably stuff like that should be avoided. Minimally cooked foods, or fresh foods would have a minimum of this toxic cholesterol derivative. So indeed, the way meat is cooked may be a significant way to introduce these cholesterol-oxygen problem compounds in the blood, and these are indeed soluble.
However, like most everything, there is a reason for this artery aggravating 25-hydroxycholesterol (immune response against viruses) to exist:
Armand-Frappier Outstanding Student Award--The emerging role of 25-hydroxycholesterol in innate immunity.
25-Hydroxycholesterols in innate and adaptive immunity.
There is an enzyme that responds to interferon by hydroxylating cholesterol. 25HC is antiviral.
Given that your blood levels of ApoB bound cholesterol are from your liver and not from a vat of oil boiling around for weeks, it would not cause any arterial injury. This is dependent on antioxidant functions preventing oxidation. These are enzymatic, such as PON and glutathione, and enteral/parenteral such as Vitamin C, E, and A.
Saturday, August 1, 2015
Pure cholesterol versus oxidized cholesterol and the role of antioxidants.
Now this is interesting. "Purified cholesterol at the same dose produced no effect." This painstaking chemistry is rare and goes to show that you can call something cholesterol, but it may not actually be cholesterol. All these oxygen adducts of cholesterol and other junk are very aggravating to the artery, causing "intimal, fibrous lesions without foam cells or hypercholesterolemia" the sort of thing you might see in advanced scorbutic lesions of the artery wall. This probably pertains to cheap Vitamin C too, which might contain some harmful junk. Pure Vitamin C of good quality, not questionable and impure, is probably as important.
Arch Pathol Lab Med. 1976 Nov;100(11):565-72. Angiotoxicity and arteriosclerosis due to contaminants of USP-grade cholesterol. Imai H, Werthessen NT, Taylor CB, Lee KT. Abstract Impurities were concentrated from several lots of cholesterol by recrystallizing cholesterol from methanol solution, retaining the mother liquor, and evaporating the residuum to dryness under vacuum. This concentrate contained the products of spontaneous oxidation of cholesterol and other contaminants from the original source. The concentrate increased the frequency of dead aortic smooth muscle cells and induced focal intimal edema in the rabbit 24 hours after gavage at 250 mg/kg. New or old cholesterol was similarly angiotoxic, the old more so than the new. Cholesterol purified via dibromination induced an increase in aggregate debris in 24 hours at 250 mg/kg but no increase in degenerated cells. The concentrate administered at a total dose of 1 gm/kg/seven weeks induced intimal, fibrous lesions without foam cells or hypercholesterolemia. Purified cholesterol at the same dose produced no effect.
The problem with food is that unless you keep it under nitrogen and don't cook any of your food, invariably there will be some oxidized cholesterol products. My arteries balk at the sight of this crud. The good news is that unlike the experimental condition above and in other experiments adding oxidized cholesterol, there isn't a whole lot of it in what you eat unless you exclusively eat low quality fast food that is fried the hell out of in oil that recirculates and boils in the air for sometimes weeks at a time, which is like an oxidation factory. Then you might worry some about oxidized cholesterol.
The good news is that there is an enzyme that can prevent LDL oxidation called paraoxonase.
Paraoxonase active site required for protection against LDL oxidation involves its free sulfhydryl group and is different from that required for its arylesterase/paraoxonase activities: selective action of human paraoxonase allozymes Q and R.
The reality is that cardiovascular disease is rampant in industrialized nations where there is plenty of fruits and vegetables available 365 days a year. If apples and oranges were the cure for heart disease, there would be no heart disease in the US. By logical deduction, it is not a lack of orange or apple, but something else.
Like a broken record, many scientists the world over have implicated that the human need for Vitamin C and other essential nutrients is much greater than what the RDA maintains, and unfortunately what food can deliver. Unless we all start eating a whole bunch of acerola cherries all the time, for example, you would need to eat 30 oranges a day or drink the equivalent of fresh squeezed juice to get a modest 2.7 grams of ascorbate. The whole point of the idea of vitamins was to cover what nutritious food, like oranges and apples could not provide, especially given that trees only fruit 3-5 months a year, leaving humans ravaged by scurvy during the non-fruiting season, therefore creating the situation "cyclical scurvy." When Vitamin C containing fruits and vegetables are available in the growing season again, the atherosclerosis accelerates during this period, not reduces, in order to build a more scurvy resistant arterial wall. You want to have a consistent optimal dose at all times.
Now that was a tangent, but not really, as serum antioxidants like Vitamin C have everything to do with preventing cholesterol oxidation and enhancing PON function. The understated and amazing observation made in 1976 is that purified cholesterol, free of oxidation products and contaminants, is harmless to the artery wall.
Arch Pathol Lab Med. 1976 Nov;100(11):565-72. Angiotoxicity and arteriosclerosis due to contaminants of USP-grade cholesterol. Imai H, Werthessen NT, Taylor CB, Lee KT. Abstract Impurities were concentrated from several lots of cholesterol by recrystallizing cholesterol from methanol solution, retaining the mother liquor, and evaporating the residuum to dryness under vacuum. This concentrate contained the products of spontaneous oxidation of cholesterol and other contaminants from the original source. The concentrate increased the frequency of dead aortic smooth muscle cells and induced focal intimal edema in the rabbit 24 hours after gavage at 250 mg/kg. New or old cholesterol was similarly angiotoxic, the old more so than the new. Cholesterol purified via dibromination induced an increase in aggregate debris in 24 hours at 250 mg/kg but no increase in degenerated cells. The concentrate administered at a total dose of 1 gm/kg/seven weeks induced intimal, fibrous lesions without foam cells or hypercholesterolemia. Purified cholesterol at the same dose produced no effect.
The problem with food is that unless you keep it under nitrogen and don't cook any of your food, invariably there will be some oxidized cholesterol products. My arteries balk at the sight of this crud. The good news is that unlike the experimental condition above and in other experiments adding oxidized cholesterol, there isn't a whole lot of it in what you eat unless you exclusively eat low quality fast food that is fried the hell out of in oil that recirculates and boils in the air for sometimes weeks at a time, which is like an oxidation factory. Then you might worry some about oxidized cholesterol.
The good news is that there is an enzyme that can prevent LDL oxidation called paraoxonase.
Paraoxonase active site required for protection against LDL oxidation involves its free sulfhydryl group and is different from that required for its arylesterase/paraoxonase activities: selective action of human paraoxonase allozymes Q and R.
The reality is that cardiovascular disease is rampant in industrialized nations where there is plenty of fruits and vegetables available 365 days a year. If apples and oranges were the cure for heart disease, there would be no heart disease in the US. By logical deduction, it is not a lack of orange or apple, but something else.
Like a broken record, many scientists the world over have implicated that the human need for Vitamin C and other essential nutrients is much greater than what the RDA maintains, and unfortunately what food can deliver. Unless we all start eating a whole bunch of acerola cherries all the time, for example, you would need to eat 30 oranges a day or drink the equivalent of fresh squeezed juice to get a modest 2.7 grams of ascorbate. The whole point of the idea of vitamins was to cover what nutritious food, like oranges and apples could not provide, especially given that trees only fruit 3-5 months a year, leaving humans ravaged by scurvy during the non-fruiting season, therefore creating the situation "cyclical scurvy." When Vitamin C containing fruits and vegetables are available in the growing season again, the atherosclerosis accelerates during this period, not reduces, in order to build a more scurvy resistant arterial wall. You want to have a consistent optimal dose at all times.
Now that was a tangent, but not really, as serum antioxidants like Vitamin C have everything to do with preventing cholesterol oxidation and enhancing PON function. The understated and amazing observation made in 1976 is that purified cholesterol, free of oxidation products and contaminants, is harmless to the artery wall.
Saturday, July 4, 2015
The Vast Need of The Human Carriage and Why Synthetic Vitamins, Especially Synthetic Vitamin C Is Necessary.
Everybody needs to run away from romantic delusions of two sorts.
One the pathetic crypto-Nazi sentiment that they or a population of humanity does not need as much Vitamin C. Given that the predicted human lifespan should easily be 150 years with vigor and youth retained at age 100, this is a laughable retrospective delusion. There is not a person on Earth who doesn't need to rescue their genetic defect in their L-Gulono-y-lactone oxidase gene. Nordic, Germanic, whatever. It doesn't include you either. You still need multi-gram quantities of ascorbate through your entire life without cessation.
The other, a naturalist idea, that we must succumb to our biological frailties because we are supposed to have them. Then there is no point to medical science and progress. It is akin to a sort of suicide, philosophical at its core, but in action a suicide. Science is intrinsically artificial and synthetic. Not everything of nature is good for humans. The loss of Vitamin C synthesis, for example, was intended to cripple humanity. Natural and Synthetic are not synonymous with "Good" and "Bad." We must wipe this illogical association from our minds. A Toshiba computer is what? Natural??
We are obliged to respect and preserve The Earth and its pristine ecologies, unpoisoned by Man, but this may also take technology to do so.
The premise is and always will be that several grams of ascorbate a day are necessary to prevent and treat human cardiovascular diseases. It is not the only element necessary. The human physiology is vastly needy with many biochemical auxotrophies crippling it, not just the Gulo gene absence. If we were replete with these substances, we would be like plants, just needing mineral water, sunshine, and carbon dioxide. We're not plants. Humans take tremendous and vast resources to support on a physiological level, but we wouldn't be the most resource intensive mammal. Certain whales take enormous food resources.
Why pretend we don't need exactly what we need? Knowing that say 4 grams of ascorbate is what all humans need minimally per day to stall or prevent heart attacks and strokes, that would mean the equivalent of Vitamin C contained in 40 oranges...a day. Is it practical to rely on orange tree or lemon tree orchards to prevent heart disease and cancer? To cut to the chase, NO. Not for us, a mammal that has been GENETICALLY HANDICAPPED. All humans possess this defect, so no proud want-to-be Nazi can gloat that they need less Vitamin C than their "lesser" peer.
Let's break it down in real-life terms and show why it is exactly about "vitamin pills." You cannot rely on vitamin pill sales and then claim that it "isn't about vitamin pills." Without the commerce element, it is ever about vitamin pills to save the human race from suffering.
Orange Orchard Logistics 101 - You need to learn this before making some stupid, embarrassing global claim about planting oranges everywhere.
 In a "high density" orchard, consisting of one acre, nevermind water requirement, there are 1500 orange trees. Each will produce 300 oranges per tree at year 5, for a total of 450,000 oranges per year on one acre. Remember, this is land that is dedicated to orange and nothing and nobody else. Minus the juice, that is 45,000 grams of ascorbate per year. It seems like a great deal, but let's break it down further given real world parameters. Given ALL adults require MINIMALLY 4 grams a day, everyday for prevention of major disease, this breaks down to 45,000/4grams a day/365 days a year = Less than 31 people.
In a "high density" orchard, consisting of one acre, nevermind water requirement, there are 1500 orange trees. Each will produce 300 oranges per tree at year 5, for a total of 450,000 oranges per year on one acre. Remember, this is land that is dedicated to orange and nothing and nobody else. Minus the juice, that is 45,000 grams of ascorbate per year. It seems like a great deal, but let's break it down further given real world parameters. Given ALL adults require MINIMALLY 4 grams a day, everyday for prevention of major disease, this breaks down to 45,000/4grams a day/365 days a year = Less than 31 people.
This is less than needed to keep 31 people healthy.
The population of Europe was 742,500,000 people in 2013. In order to indirectly and inefficiently make 4 grams of Vitamin C for all these individuals per year, you would need a citrus orchard of 23,951,612 acres size. This translates to 37,500 square miles of orchard or greater than the size of Wisconsin.
Given that this is feasible, and certainly there are that many orange orchards, why hasn't orange juice saved humanity from atherosclerosis?
There are about 8 oranges in a big 16 oz cup of juice, or two glasses of juice. This would be 800 mg of Vitamin C, a good beneficial dose, but hardly enough to get to the therapeutic amount of 40 oranges a day, or 5 big glasses of orange juice (plus the sugars) EVERYDAY. Not only does nobody do this, it is not tolerable. As delicious as it is, nobody can stomach such enormous quantities of orange juice. Attempting to EAT 40 oranges EVERYDAY is even worse. If you are talking apples, we're talking ten times more apples - FOUR HUNDRED APPLES A DAY = 3.4 grams Vitamin C.
Only a concentrated extract taken undiluted would be and could be effective, and this would take...SCIENCE AND TECHNOLOGY to squeeze the nutrition of 400 apples into a tolerable volume! It is deceptive and irresponsible to suggest that eating an orange or an apple a day will stave off the genetic defect all humans possess in some kind of romantic naturalism statement on behalf of somebody who does not take their vitamins, like a child who won't eat their vegetables. There is an easier solution in place, synthetic but good and pure Vitamin C, also a product of science. Naturalism, the human notion, is not always constructive or forward looking. It can plunge you backwards to square one.
One the pathetic crypto-Nazi sentiment that they or a population of humanity does not need as much Vitamin C. Given that the predicted human lifespan should easily be 150 years with vigor and youth retained at age 100, this is a laughable retrospective delusion. There is not a person on Earth who doesn't need to rescue their genetic defect in their L-Gulono-y-lactone oxidase gene. Nordic, Germanic, whatever. It doesn't include you either. You still need multi-gram quantities of ascorbate through your entire life without cessation.
The other, a naturalist idea, that we must succumb to our biological frailties because we are supposed to have them. Then there is no point to medical science and progress. It is akin to a sort of suicide, philosophical at its core, but in action a suicide. Science is intrinsically artificial and synthetic. Not everything of nature is good for humans. The loss of Vitamin C synthesis, for example, was intended to cripple humanity. Natural and Synthetic are not synonymous with "Good" and "Bad." We must wipe this illogical association from our minds. A Toshiba computer is what? Natural??
We are obliged to respect and preserve The Earth and its pristine ecologies, unpoisoned by Man, but this may also take technology to do so.
The premise is and always will be that several grams of ascorbate a day are necessary to prevent and treat human cardiovascular diseases. It is not the only element necessary. The human physiology is vastly needy with many biochemical auxotrophies crippling it, not just the Gulo gene absence. If we were replete with these substances, we would be like plants, just needing mineral water, sunshine, and carbon dioxide. We're not plants. Humans take tremendous and vast resources to support on a physiological level, but we wouldn't be the most resource intensive mammal. Certain whales take enormous food resources.
Why pretend we don't need exactly what we need? Knowing that say 4 grams of ascorbate is what all humans need minimally per day to stall or prevent heart attacks and strokes, that would mean the equivalent of Vitamin C contained in 40 oranges...a day. Is it practical to rely on orange tree or lemon tree orchards to prevent heart disease and cancer? To cut to the chase, NO. Not for us, a mammal that has been GENETICALLY HANDICAPPED. All humans possess this defect, so no proud want-to-be Nazi can gloat that they need less Vitamin C than their "lesser" peer.
Let's break it down in real-life terms and show why it is exactly about "vitamin pills." You cannot rely on vitamin pill sales and then claim that it "isn't about vitamin pills." Without the commerce element, it is ever about vitamin pills to save the human race from suffering.
Orange Orchard Logistics 101 - You need to learn this before making some stupid, embarrassing global claim about planting oranges everywhere.

This is less than needed to keep 31 people healthy.
The population of Europe was 742,500,000 people in 2013. In order to indirectly and inefficiently make 4 grams of Vitamin C for all these individuals per year, you would need a citrus orchard of 23,951,612 acres size. This translates to 37,500 square miles of orchard or greater than the size of Wisconsin.
Given that this is feasible, and certainly there are that many orange orchards, why hasn't orange juice saved humanity from atherosclerosis?
There are about 8 oranges in a big 16 oz cup of juice, or two glasses of juice. This would be 800 mg of Vitamin C, a good beneficial dose, but hardly enough to get to the therapeutic amount of 40 oranges a day, or 5 big glasses of orange juice (plus the sugars) EVERYDAY. Not only does nobody do this, it is not tolerable. As delicious as it is, nobody can stomach such enormous quantities of orange juice. Attempting to EAT 40 oranges EVERYDAY is even worse. If you are talking apples, we're talking ten times more apples - FOUR HUNDRED APPLES A DAY = 3.4 grams Vitamin C.
Only a concentrated extract taken undiluted would be and could be effective, and this would take...SCIENCE AND TECHNOLOGY to squeeze the nutrition of 400 apples into a tolerable volume! It is deceptive and irresponsible to suggest that eating an orange or an apple a day will stave off the genetic defect all humans possess in some kind of romantic naturalism statement on behalf of somebody who does not take their vitamins, like a child who won't eat their vegetables. There is an easier solution in place, synthetic but good and pure Vitamin C, also a product of science. Naturalism, the human notion, is not always constructive or forward looking. It can plunge you backwards to square one.
Atherosclerosis Is Not A Modern Disease. Lifespan Was Shorter Not Longer In Ancient Humans.
Looking at atherosclerotic plaque in people 4000 years ago.
Today we are awash with paleo diet recommendations or vegetarian/granarian/fruitarian diets, all consumed by ancient human beings. They DIDN'T live longer, they lived much shorter lives. People never reached 50 years of age, and this age was correlated with rampant atherosclerosis (plaque). They certainly had orange and apple trees back then. There is no shortage of apples in Europe, so that is clearly not the cause of atherosclerosis in Europe. It is not because of an "apple tree deficiency." Our clean eating ancestors had severe atherosclerosis before the age of 40. Why could this be? They ate plenty of apples...
The German and Norse Pagan festivals featured many many apples (to eat). "Brita as Iduna" (1901) by Carl Larsson:

We have a heritable in-born genetic defect of ascorbate synthesis that goes beyond just a sprinkle or dash. It was the great pioneers such as Pauling, Stone, Cameron, Willis, who initiated the idea of megadose ascorbate consumption (which is not mega but actually normal). The schizophrenic contradiction of wanting this threshold rescue dose of this genetic defect to be lower by the day is pure insanity. It is like saying one day humans will not need to drink several glasses of water a day to be alive. It "ain't gonna happen." The orange tree idea takes us to square one, as the therapeutic dose for atherosclerosis is minimally 4,000 mg ascorbate. That is 40 oranges, more than a tree may make all year. Until the day we as a species actually genetically engineer back a working copy (is this natural?) to replace our corrupted yet present Gulo gene, we will need to take in effective amounts of the rescue substance, ascorbate.
That is the whole idea behind science, the mastery of our biological weaknesses, and so called "vitamins." If we are naturalists to the extreme, throw away your computer, wear burlap sacks, live like a Quaker and we can forget about vitamin pills altogether, plunging ourselves all the way back to 4000 years ago where people were rife with atherosclerosis and lived to a little over 40 years of age despite "perfect" natural diets with no fried or packaged foods.
It's the missing substances, stupid.
Sunday, June 7, 2015
Lipoprotein(a) and macrophages in tandem within a human coronary plaque biopsy:

The question of causality and time-frame is always to question. The essential point we're trying to make is that Lp(a) doesn't just swoop in from out of nowhere for no reason all the sudden. Macrophages which do home into inflammatory cytokine signals emitted by the artery, and do burrow in to receive cholesterol via active receptor exchange to return to the liver, also don't just suddenly go in and start chewing up lipoproteins. That being said, foam cells and Lp(a) happen together frequently. In any remodeling process in the body, there is nearly certainly found macrophages. You can't just ignore the immune system.
What is my position? It is irrelevant. It is beyond irrelevant "who is right," but what is germaine is "WHAT is right." I do not care "who" is right, nor should you. Those who care intensely about who should be right obviously have something else driving them like a jerk's ego or some frivolous vendetta. The question should be, how do we make each and every one of the millions of people of Earth right in their application of science. What we should all care about is "what is right," not "who is right." Needless to say, that is my concern in science, no extraneous nonsense.
What is true is that macrophages are initially participating in a beneficial remodeling process, and not chewing up ox-LDL in some parasitic process, but attempting to hand back the remodeling waste, the construction site debris back to the liver for recycling via....HDL. We certainly can't ignore HDL in this repair process either. It will spin cardiopathology's noodle when they see that the majority of atherosclerotic plaques are rich in ApoE, which if extended the old logic applied to LDL is causing harmful things. On the contrary, the presence of ApoE we all know to be part of the repair process which may be overwhelmed by a net excess of damage as opposed to a net excess of repair.
Does Lp(a) cause atherosclerosis? Only if there is a reason for atherosclerosis to take place. For a many humans who eat just an orange a day but still have the Gulo-/- genetic defect, there is a lot of cumulative damage that does occur which needs patching by Lp(a) and the coagulation system. Think of it this way, when thinking about preserving arterial integrity: a normal rat makes the equivalent of 5 grams a day in a 70 kilo human when nothing is going on. In stressful times, a rat makes 300% more vitamin C. This entry certainly is not encouraging or supporting the fallacy that dietary cholesterol causes heart disease. It does not, but other dietary factors such as too low vitamin C, B, E, magnesium, K, D, amino acids and too much trans-fatty acids and omega-6 do. The recent US Federal guidance to stop paying attention to ingested cholesterol is a well-studied one made with decades of clinical evidence that cholesterol consumption has historically had nothing to do with the rate of heart disease.
I think this statement I made a long time ago sums it up nicely about what is going on:
"A big lump is better than a big hole."
One prevents lethal hemorrhage, the most dramatic example in human biology being the aortic dissection with adventitial failure, the other is lethal hemorrhage. One of the first priorities of the human physiology is to stop bleeding and hemorrhaging. It drops everything it is doing and attends to that first, even if it means making a pile of disorganized stuff at the site of leaking that is harmful down the road. Better than bleeding to death. Lp(a) is very atherogenic at sites of arterial damage, and sticks more to the glycocalyx with ascending concentrations. If the endothelium is in tact, there is nothing for Lp(a) to react to, no ligand, no binding site to the ligand. Lp(a) just floats along harmlessly as it does not encounter plasminogen binding sites, free lysyls, fibrin, exposed subendothelial fibronectin, etc. You can't just ignore the coagulation system either. Lp(a) has a direct affinity to fibrin(ogen) which is Clotting Factor 1, and gets cross-linked to fibrin clots via FactorXIII. Do macrophages foam cells CAUSE atherosclerosis? No. They are attempting to prevent it, but the process can and does go wrong if they get overwhelmed. When they are participating in arterial repair, foam cells are formally defined as early plaques, but that is simply a matter of scientific semantics. Perhaps one day, they will be relabeled as "reparative cells" distinct from a fibrofatty mass devoid of cells that can rupture and cause thrombosis. Given an equal sized foam cell lesion and fibrofatty mass with thin cap that is less than 20% occlusive, the unstable fibrofatty mass is the dangerous thing, and the foam cell lesion is unconcerning.
Macrophages and foam cells are not always in human atherosclerotic plaques. In fact, many times, they are not there at all. Many pathologist specimens of human diseased atherosclerotic arteries do not have foam cells, which is why some scientists choose to de-emphasize them or diminish their importance. But they do happen, and we can't just ignore them. One improvement in the future state-of-the-art may be to put macrophages and foam cell "lesions" in a category all on their own as they are dynamically different from all other component atherosclerotic plaques, and not just different in cellular origin and composition. They also serve an entirely different purpose altogether than other cells found in human plaques, including remodeling, debris clearance, and returning the artery back to its original state.
Saturday, June 6, 2015
You can't just ignore foam cells. Fatty streaks happen, with or without Lp(a). An addendum of "Common Sense."
Given that the guinea pig DOES NOT have Lp(a) but only LDL in a higher ratio to HDL than in wild mice, and that they do incur atherosclerosis upon chronic scurvy, there is no ambiguity that vitamin C deficiency is causal to atherosclerosis WITHOUT invoking apo(a). Unless a genetically modified variant of guinea pig happens, they will never express apo(a) protein. The "immunological evidence" proferred by others is obviously a cross-reaction to a different protein, perhaps even apo(a)-like, but certainly it is not lipoprotein(a). It could not be, rendering any reference to Lp(a) an illogical train of thinking. However, they do have an ample amount of LDL. ApoB particles are important to atherogenesis. We can't just suddenly start ignoring ApoB, not the Lp(a) platform people either. Without ApoB synthesis, amplified by inflammatory arterial cytokines, there is NO Lp(a). In mice that can't make vitamin C but also don't have much LDL but a vast majority of HDL, atherosclerosis is limited to a mild physiological hypertrophy, proteoglycan accumulation, and fibrosis, called arteriosclerosis in olden days. There are some thoracic aortic lesions especially at bifurcations to the digestive system, but little to no atheroma of any visible or clinically significant nature with a majority HDL and few ApoB particles/absolute mass/LDL-cholesterol. This clearly shows that ApoB containing particles outnumbering ApoA containing particles is a precondition to scurvy induced atherosclerosis, as much as scurvy is a precondition to endothelial dysfunction, the cause and initiation of most atherosclerosis. This is without getting into the complicated vasa vasorum component which later contributes to erythrocyte evasation into pre-existing plaques where they die and rupture, releasing membrane cholesterol and iron. (It may be in the very near future, the lipid cores and free cholesterol are found to be from intra-plaque hemorrhage from the interdigitating vasa vasorum rather than the vexing (to some people) foam cell plaque "bust.")
That being said, the atherosclerosis that occurs without Lp(a) is much milder than that which occurs with Lp(a). Atherosclerosis with low Lp(a) and human-esque levels of LDL is much decreased in lesion number, lesion size, and lesion complexity compared to atherosclerosis that occurs with even moderate Lp(a) around. Lp(a) over 30mg/dL certainly will drive more atherosclerosis, but lower levels of Lp(a) below 20mg/dL also contribute by virtue of its "homing missile" like quality of binding to areas of damage which it finds in the system circulation of 60,000 miles. It may not matter how much over a certain threshold of Lp(a), but it does potentiate worse and more with ascending blood levels of Lp(a). There is no question that Lp(a) is atherogenic, but without LDL, how can there be Lp(a)? It is not an "either-or" or "better or worse" proposition, but where all these facts that the 1000's of highly intelligent global cardiology scientists have seen intersect and what that nexus and conjunction of truth is.
Ox-LDL is a reliable marker of vessel disease and number of vessel involvement
Does this mean that Ox-LDL causes atherosclerosis? Yes AND No. It is too low to ever cause atherosclerosis, with circulating levels in multi-vessel CAD being at most 4mg/dL, and normally being 1mg/dL. However, it is an extremely reliable indicator of CAD, with a level of 3mg/dL Ox-LDL most certainly revealing plaque in the coronaries somewhere. Its importance is locally in microenvironments where inflammation causes ROS which causes oxidation and acetylation of LDL in the microscopic milieu around the lesion. If LDL is not oxidized or denatured, it is not "irritating" to the artery, no. Regular LDL, even in very high concentrations has been proven not to be cytotoxic to the endothelial cell or cause stress fiber contraction. As I have already said a long time ago, the LDL gets into the artery if and when the endothelial layer (or vasa vasorum) is compromised and has spatially large enough breaches for it to go through. Vesicular transport would cause LDL to accumulate inside a cell, not outside it, which we'll get to in just a second.
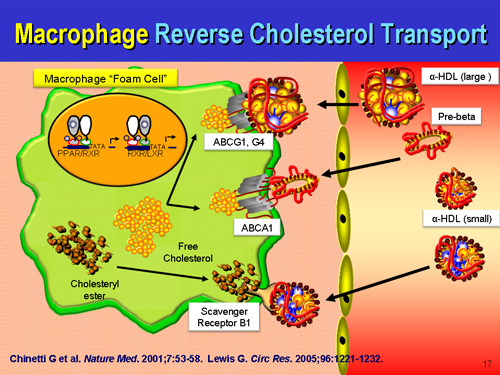
LDL consumption by a cell is highly regulated, and a cell stops internalizing LDL when it has enough, or the cell will turn down its internal synthesis while maintaining internalization. Extracellular aggregates of native LDL could not be there if they could not reach these subendothelial compartments somehow (increased vascular permeability). Ox-and Ac-LDL has a special receptor, scavenger receptor, evolutionarily built in humans, the creature with nearly exclusively the majority of fatal heart attacks and strokes, to get rid of apoptotic cells...and denatured LDL. When scavenger receptor cells encounter ox-LDL, they engulf it without stop. Call it gobbling, but more accurately, they are the "trash men," the "recycling team," not "police men." As much as a policeman can clear debris on a highway, and often does for the public benefit, the macrophage can also serve to clean the artery, not "eat it" or "police" it. The "old concept" people know that fatty streaks, cellular foam cell masses DO NOT burst. So, the cartoon does call out an inaccuracy - the notion that foam cell lesions form, burst open, and evulse their cholesterol into the artery. Early on, no. These are most stable cellular accumulations which would prevent further destabilization of an artery. Later on, if the condition is unresolved, the damage unmended, and the "artery tumor" becomes hypoxic, like in a tumor, the macrophages would undergo necrosis and form a necrotic core, just like happens in a tumor core.
In human plaques, foam cell formation from the smooth muscle cell component is vastly underestimated because in mice, the majority of foam cells occur from macrophages. In humans a greater proportion of foam cells happen from the artery cells themselves. Yet, make no mistake, foam cell "fatty streaks" are found all the time in human atherosclerosis. They may be there, they may not be, but an astute scientist does not simply ignore foam cells, especially those colocalized upon an Lp(a) deposit. There are vastly more human plaques that do not have a foam cell component, and these actually are more worrisome because they are less revertible than a foam cell fatty streak. Why?
The foam cell, like the apo(a) protein, isn't just some random superfluous curiosity, an accident of biology with no purpose. Foam cells not only contribute to the artery structure temporarily as additional cells with their hydrophobic seal against hemorrhage, cholesterol, but also are participating in transport of excess unused or remaining cholesterol back to the liver, just as LDL delivers useful cholesterol for cell replacement. Of all cell types, the macrophage is very efficient at this process. So we see that this too is a useful, purposeful event, that if resolves satisfactorily, signals the macrophages to exit the artery wall, making the fatty streak lump vanish. Some call it "reverse cholesterol transport," others don't like that name and call it something else. Once again, you can't just ignore foam cells or dismiss fatty streaks. Just as Goldstein and Brown didn't just fabricate a mythic fable of LDL homeostasis, despite this encouraging systemic statin poisoning, scientists and pathologists did not 'just make up' a fable of fatty streaks and foam cells being in human arteries. Truly, these are about repair, rather than a nonsensical auto-attack on the artery wall, although auto-immune arteritis is a real disease too. It is increasingly important to stay updated with the field to see others' understanding of the issue so that all science and scientists everywhere can eventually come to a real-world consensus. Or we can rage around ham-fisted and grandstanding, pretending to know everything without the diligence necessary to know everything.
Macrophage reverse cholesterol transport: key to the regression of atherosclerosis?




That being said, the atherosclerosis that occurs without Lp(a) is much milder than that which occurs with Lp(a). Atherosclerosis with low Lp(a) and human-esque levels of LDL is much decreased in lesion number, lesion size, and lesion complexity compared to atherosclerosis that occurs with even moderate Lp(a) around. Lp(a) over 30mg/dL certainly will drive more atherosclerosis, but lower levels of Lp(a) below 20mg/dL also contribute by virtue of its "homing missile" like quality of binding to areas of damage which it finds in the system circulation of 60,000 miles. It may not matter how much over a certain threshold of Lp(a), but it does potentiate worse and more with ascending blood levels of Lp(a). There is no question that Lp(a) is atherogenic, but without LDL, how can there be Lp(a)? It is not an "either-or" or "better or worse" proposition, but where all these facts that the 1000's of highly intelligent global cardiology scientists have seen intersect and what that nexus and conjunction of truth is.
Ox-LDL is a reliable marker of vessel disease and number of vessel involvement
Does this mean that Ox-LDL causes atherosclerosis? Yes AND No. It is too low to ever cause atherosclerosis, with circulating levels in multi-vessel CAD being at most 4mg/dL, and normally being 1mg/dL. However, it is an extremely reliable indicator of CAD, with a level of 3mg/dL Ox-LDL most certainly revealing plaque in the coronaries somewhere. Its importance is locally in microenvironments where inflammation causes ROS which causes oxidation and acetylation of LDL in the microscopic milieu around the lesion. If LDL is not oxidized or denatured, it is not "irritating" to the artery, no. Regular LDL, even in very high concentrations has been proven not to be cytotoxic to the endothelial cell or cause stress fiber contraction. As I have already said a long time ago, the LDL gets into the artery if and when the endothelial layer (or vasa vasorum) is compromised and has spatially large enough breaches for it to go through. Vesicular transport would cause LDL to accumulate inside a cell, not outside it, which we'll get to in just a second.
LDL consumption by a cell is highly regulated, and a cell stops internalizing LDL when it has enough, or the cell will turn down its internal synthesis while maintaining internalization. Extracellular aggregates of native LDL could not be there if they could not reach these subendothelial compartments somehow (increased vascular permeability). Ox-and Ac-LDL has a special receptor, scavenger receptor, evolutionarily built in humans, the creature with nearly exclusively the majority of fatal heart attacks and strokes, to get rid of apoptotic cells...and denatured LDL. When scavenger receptor cells encounter ox-LDL, they engulf it without stop. Call it gobbling, but more accurately, they are the "trash men," the "recycling team," not "police men." As much as a policeman can clear debris on a highway, and often does for the public benefit, the macrophage can also serve to clean the artery, not "eat it" or "police" it. The "old concept" people know that fatty streaks, cellular foam cell masses DO NOT burst. So, the cartoon does call out an inaccuracy - the notion that foam cell lesions form, burst open, and evulse their cholesterol into the artery. Early on, no. These are most stable cellular accumulations which would prevent further destabilization of an artery. Later on, if the condition is unresolved, the damage unmended, and the "artery tumor" becomes hypoxic, like in a tumor, the macrophages would undergo necrosis and form a necrotic core, just like happens in a tumor core.
In human plaques, foam cell formation from the smooth muscle cell component is vastly underestimated because in mice, the majority of foam cells occur from macrophages. In humans a greater proportion of foam cells happen from the artery cells themselves. Yet, make no mistake, foam cell "fatty streaks" are found all the time in human atherosclerosis. They may be there, they may not be, but an astute scientist does not simply ignore foam cells, especially those colocalized upon an Lp(a) deposit. There are vastly more human plaques that do not have a foam cell component, and these actually are more worrisome because they are less revertible than a foam cell fatty streak. Why?
The foam cell, like the apo(a) protein, isn't just some random superfluous curiosity, an accident of biology with no purpose. Foam cells not only contribute to the artery structure temporarily as additional cells with their hydrophobic seal against hemorrhage, cholesterol, but also are participating in transport of excess unused or remaining cholesterol back to the liver, just as LDL delivers useful cholesterol for cell replacement. Of all cell types, the macrophage is very efficient at this process. So we see that this too is a useful, purposeful event, that if resolves satisfactorily, signals the macrophages to exit the artery wall, making the fatty streak lump vanish. Some call it "reverse cholesterol transport," others don't like that name and call it something else. Once again, you can't just ignore foam cells or dismiss fatty streaks. Just as Goldstein and Brown didn't just fabricate a mythic fable of LDL homeostasis, despite this encouraging systemic statin poisoning, scientists and pathologists did not 'just make up' a fable of fatty streaks and foam cells being in human arteries. Truly, these are about repair, rather than a nonsensical auto-attack on the artery wall, although auto-immune arteritis is a real disease too. It is increasingly important to stay updated with the field to see others' understanding of the issue so that all science and scientists everywhere can eventually come to a real-world consensus. Or we can rage around ham-fisted and grandstanding, pretending to know everything without the diligence necessary to know everything.
Macrophage reverse cholesterol transport: key to the regression of atherosclerosis?



Sunday, February 1, 2015
Collagen IV derived "tumstatin" suppresses tumor growth.
Collagen IV, the basement membrane collagen is probably one of the oldest and most examined subtypes of collagen in oncology. It is certainly not the only or most important collagen in cancer suppression, or other diseases, but Col4 has been proven to function as a barrier against metastasis in the fibrous capsule in several sophisticated and technically up-to-date studies.
Growing tumors develop additional new blood vessels to meet the demand for adequate nutrients and oxygen, a process called angiogenesis. Cancer is a highly complex disease promoted by excess angiogenesis; interfering with this process poses for an attractive approach for controlling tumor growth. This hypothesis led to the identification of endogenous angiogenesis inhibitors generated from type IV collagen, a major component of vascular basement membrane (VBM). Type IV collagen and the angiogenesis inhibitors derived from it are involved in complex roles, than just the molecular construction of basement membranes. Protease degradation of collagens in VBM occurs in various physiological and pathological conditions and produces several peptides. Some of these peptides are occupied in the regulation of functions conflicting from those of their original integral molecules. Tumstatin (alpha3(IV)NC1), a proteolytic C-terminal non-collagenous (NC1) domain from type IV collagen alpha3 chain has been highlighted recently because of its potential role in anti-angiogenesis, however its biological actions are not limited to these processes. alpha3(IV)NC1 inhibits proliferation by promoting endothelial cell apoptosis and suppresses diverse tumor angiogenesis, thus making it a potential candidate for future cancer therapy. The present review surveys the physiological functions of type IV collagen and discovery of alpha3(IV)NC1 as an antiangiogenic protein with a comprehensive overview of the knowledge gained by us towards understanding its signaling mechanisms."
Inhibition of tumor angiogenesis by tumstatin: insights into signaling mechanisms and implications in cancer regression.
"Sudhakar A1, Boosani CS.Growing tumors develop additional new blood vessels to meet the demand for adequate nutrients and oxygen, a process called angiogenesis. Cancer is a highly complex disease promoted by excess angiogenesis; interfering with this process poses for an attractive approach for controlling tumor growth. This hypothesis led to the identification of endogenous angiogenesis inhibitors generated from type IV collagen, a major component of vascular basement membrane (VBM). Type IV collagen and the angiogenesis inhibitors derived from it are involved in complex roles, than just the molecular construction of basement membranes. Protease degradation of collagens in VBM occurs in various physiological and pathological conditions and produces several peptides. Some of these peptides are occupied in the regulation of functions conflicting from those of their original integral molecules. Tumstatin (alpha3(IV)NC1), a proteolytic C-terminal non-collagenous (NC1) domain from type IV collagen alpha3 chain has been highlighted recently because of its potential role in anti-angiogenesis, however its biological actions are not limited to these processes. alpha3(IV)NC1 inhibits proliferation by promoting endothelial cell apoptosis and suppresses diverse tumor angiogenesis, thus making it a potential candidate for future cancer therapy. The present review surveys the physiological functions of type IV collagen and discovery of alpha3(IV)NC1 as an antiangiogenic protein with a comprehensive overview of the knowledge gained by us towards understanding its signaling mechanisms."
Tumstatin, the NC1 domain of alpha3 chain of type IV collagen, is an endogenous inhibitor of pathological angiogenesis and suppresses tumor growth.
"
Angiogenesis,
the formation of new blood vessels, is required for physiological
development of vertebrates and repair of damaged tissue, but in the
pathological setting contributes to progression of cancer. During tumor
growth, angiogenesis is supported by up-regulation of angiogenic
stimulators (pro-angiogenic) and down-regulation of angiogenic
inhibitors (anti-angiogenic). The switch to the angiogenic phenotype
(angiogenic switch) allows the tumors to grow and facilitate metastasis.
The bioactive NC1 domain of type IV collagen
alpha3 chain, called tumstatin, imparts anti-tumor activity by inducing
apoptosis of proliferating endothelial cells. Tumstatin binds to
alphaVbeta3 integrin via a mechanism independent of the RGD-sequence
recognition and inhibits cap-dependent protein synthesis in the
proliferating endothelial cells. The physiological level of tumstatin is
controlled by matrix metalloproteinase-9, which most effectively
cleaves it from the basement membrane and its physiological
concentration in the circulation keeps pathological angiogenesis and
tumor growth in check. These findings suggest that tumstatin functions
as an endogenous inhibitor of pathological angiogenesis and functions as
a novel suppressor of proliferating endothelial cells and growth of
tumors."
Collagen XIX is strongly anti-tumorigenic
The NC1 domain of type XIX collagen inhibits in vivo melanoma growth.
Mol Cancer Ther. 2007 Feb;6(2):506-14.
The NC1 domain of type XIX collagen inhibits in vivo melanoma growth.
Ramont L1, Brassart-Pasco S, Thevenard J, Deshorgue A, Venteo L, Laronze JY, Pluot M, Monboisse JC, Maquart FX.
Type XIX collagen is a minor collagen
that localizes to basement membrane zones, together with types IV, XV,
and XVIII collagens. Because several NC1 COOH-terminal domains of other
chains from basement membrane collagens were reported to exhibit
antitumor activity, we decided to study the effects of the NC1(XIX) collagen
domain on tumor progression using an experimental in vivo model of
mouse melanoma. We observed a 70% reduction in tumor volume in NC1(XIX)-treated
mice compared with the corresponding controls. Histologic examination
of the tumors showed a strong decrease in tumor vascularization in
treated mice. In vitro, NC1(XIX)
inhibited the migrating capacity of tumor cells and their capacity to
invade Matrigel. It also inhibited the capacity of human microvascular
endothelial cells to form pseudotubes in Matrigel. This effect was
accompanied by a strong inhibition of membrane type-1 matrix
metalloproteinase (matrix metalloproteinase-14) and vascular endothelial
growth factor expression. Collectively, our data indicate that the NC1
domain of type XIX collagen
exerts antitumor activity. This effect is mediated by a strong
inhibition of the invasive capacities of tumor cells and antiangiogenic
effects. NC1(XIX) should now be considered as a new member of the basement membrane collagen-derived matrikine family with antitumor and antiangiogenic activity.
- PMID: 17308049
The NC1 domain of type XIX collagen inhibits melanoma cell migration.
Eur J Dermatol. 2010 Nov-Dec;20(6):712-8. doi: 10.1684/ejd.2010.1070. Epub 2010 Sep 14.
The NC1 domain of type XIX collagen inhibits melanoma cell migration.
The NC1 domain of type XIX collagen inhibits melanoma cell migration.
Type XIX collagen is a minor collagen that localizes to basement membrane zones. We previously demonstrated that the C-terminal NC1 domain of type XIX collagen inhibits tumor growth in vivo. In the present study, we analyzed the effects of the NC1(XIX) collagen domain on migratory behaviour of melanoma B16F10 cells. We found that NC1(XIX) do not inhibit melanoma cell proliferation. On the contrary, NC1(XIX)
strongly inhibited the migratory capacities of melanoma cells in the
scratch wound model and in Ibidi® devices: cell migration speed was 7.69
± 1.49 μm/h for the controls vs 6.64 ± 0.82 μm/h for cells incubated
with 30 μmol/L NC1(XIX) and 5.72 ± 0.67 μmol/h with 60 μmol/L NC1(XIX).
Similar results were obtained with UACC 903 human melanoma cells.
Further work will be necessary to elucidate the molecular mechanisms of
this migration inhibition. It may, however, explain, at least partially,
the inhibition of tumor growth that we observed in vivo.
- PMID: 20840910
Loss of Collagen XV Causes Muscle Tissue and Capillary Degeneration
Lack of type XV collagen causes a skeletal myopathy and cardiovascular defects in mice.
From:
 Muscle histology: focal areas of degeneration, regeneration, and
variation in fiber size. Hematoxylin and eosin-stained sections of the
gastrocnemius (A), triceps brachii (B),
paraspinal (C), and quadriceps (D)
muscles of 6-month-old null mice showing cell degeneration (curved
arrows, A and C) with macrophage
infiltration (A), regenerative fibers (thin arrow,
B), central nuclei (thin arrow, C), and
increased variation in fiber size with atrophic muscle fibers
(D, arrowheads) compared with age-matched wild-type mice
(E). Original magnifications: A and
D, ×300; B, ×200; C and
E, ×80.
Muscle histology: focal areas of degeneration, regeneration, and
variation in fiber size. Hematoxylin and eosin-stained sections of the
gastrocnemius (A), triceps brachii (B),
paraspinal (C), and quadriceps (D)
muscles of 6-month-old null mice showing cell degeneration (curved
arrows, A and C) with macrophage
infiltration (A), regenerative fibers (thin arrow,
B), central nuclei (thin arrow, C), and
increased variation in fiber size with atrophic muscle fibers
(D, arrowheads) compared with age-matched wild-type mice
(E). Original magnifications: A and
D, ×300; B, ×200; C and
E, ×80.
 Ultrastructural changes in capillaries. Electron microscopy of heart
capillaries from a wild-type (A) and a null mouse
(B) with swollen endothelial cells (asterisks). The
lumen is indicated by a white arrow. Skeletal muscle capillaries from a
wild-type (C) and a mutant mouse (D)
showing luminal narrowing and folding of endothelial cells.
Ultrastructural changes in capillaries. Electron microscopy of heart
capillaries from a wild-type (A) and a null mouse
(B) with swollen endothelial cells (asterisks). The
lumen is indicated by a white arrow. Skeletal muscle capillaries from a
wild-type (C) and a mutant mouse (D)
showing luminal narrowing and folding of endothelial cells.
 Effect of isoproterenol stimulation on developed pressure in
(A) 6-month-old and (B) 12-month-old
mutant and wild-type mice. The responses to β-agonists were measured
in terms of the ratio of the maximal value of the developed pressure
(DP) to the basal level before the isoproterenol perfusion in
Col15a1−/− (●:
A, n = 7; B,
n = 11) and Col15a1+/+
(□: A, n = 7;
B, n = 8) mice. The symbols
represent mean ± SEM. Significant differences between the
Col15a1−/− and
Col15a1+/+ mice are indicated by asterisks
as follows: *, P < 0.05, **,
P < 0.01. The basal pressure was 31.7 ± 5.0
and 27.3 ± 5.0 mmHg for the 6-month-old control and null mice,
respectively, and 20.2 ± 3.4 and 20.8 ± 2.0 mmHg for the
1-year-old mice (mean ± SEM).
Effect of isoproterenol stimulation on developed pressure in
(A) 6-month-old and (B) 12-month-old
mutant and wild-type mice. The responses to β-agonists were measured
in terms of the ratio of the maximal value of the developed pressure
(DP) to the basal level before the isoproterenol perfusion in
Col15a1−/− (●:
A, n = 7; B,
n = 11) and Col15a1+/+
(□: A, n = 7;
B, n = 8) mice. The symbols
represent mean ± SEM. Significant differences between the
Col15a1−/− and
Col15a1+/+ mice are indicated by asterisks
as follows: *, P < 0.05, **,
P < 0.01. The basal pressure was 31.7 ± 5.0
and 27.3 ± 5.0 mmHg for the 6-month-old control and null mice,
respectively, and 20.2 ± 3.4 and 20.8 ± 2.0 mmHg for the
1-year-old mice (mean ± SEM).
From:
Proc Natl Acad Sci U S A. 2001 Jan 30;98(3):1194-9. Epub 2001 Jan 23.
Lack of type XV collagen causes a skeletal myopathy and cardiovascular defects in mice.
Eklund L1, Piuhola J, Komulainen J, Sormunen R, Ongvarrasopone C, Fássler R, Muona A, Ilves M, Ruskoaho H, Takala TE, Pihlajaniemi T.



Sunday, January 25, 2015
Partial and Total Loss of Arterial Collagen XVIII Causes Atherosclerosis
Loss of Collagen XVIII Enhances Neovascularization and Vascular Permeability in Atherosclerosis
Some factions claim that loss of arterial collagen is causal to atherosclerosis without being very specific about the mechanism (where? the adventitia? the endothelial basement? The media? how? immune side? smc autophagic? oxidative? proteolytic? autolysis?) and refer to studies done before regarding deranged hepatic metabolism of cholesterol during scurvy which causes a certain hyperlipidemia by bile metabolism deficiency and consequent lack of fecosteroid excretion. Others will look at ratios of Collagens I, III, IV, and even V in the atherosclerotic plaque and their ratios during atherosclerosis. However, the specific mechanism of collagen loss and atherosclerosis has never been scientifically described in a definitive study until this one. Through simple logic, (common sense), it follows that singular or combinatory losses of the other arterial collagen subtypes would provide the same result experimentally, either in vitro or in vivo.
The Maeda paper showing that scurvy causes Evans Blue extravasation and gross damage to the arterial wall did not describe any atheromas, hyperplasias, or plaques because the mice die from scurvy before they can incur cumulative atherosclerosis. They did prove that scurvy causes arterial degradation to the extent that lipoproteins and anything else can enter the artery that can't transgress a healthy, vitamin C (ascorbate) replete artery wall.
The implied connection between atherosclerosis and scurvy is collagen. While ascorbate isn't the only vitamin involved in collagen synthesis, it is the only one that when absent will prevent proper polymerization of hydroxyl residues. There is nothing to debate in this regard. No ascorbate = no assembled collagen. There may be pro-collagen formation and its strands, but they will never be assembled correctly into their "stronger than steel" fibers without vitamin C, but remain a useless stockpile of components.
It is important to note that the correct ratios of the various collagens is exceedingly important. While much focus has been made on COL4 basement membranes in conferring tensile strength and resistance to metastasis, too much of COL4 without the other collagens in balance can cause mitochondrial death by integrin signaling abnormalities, as well as aberrant vitamin A processing. It is not as simple as to say "the more collagen the better." Not whatsoever is it that simple, and such a conclusion could be disastrous in clinic. Fibrosis is a disorder of too much of the wrong collagen in the wrong place at the wrong time and is a devastating disorder.
However, if the intrinsic collagens in the artery, such as COLXVIII, vanish, arteries become much more prone to lipid intrusion and the chain of events that occur after that. As such, the normal constituency of arterial collagens, many of them not even recognized by conventional histopathology stains and immunohistochemistry, prevent large particle lipoprotein intrusion. Collagen XVIII is a subtype that is virtually ignored in cardiology, yet possibly one of the most important subtypes. It logically follows that deficiencies in the most commonly acknowledged collagens of the arterial media and basement membrane, COLI, COLIII, and COLIV, would cause similar problems of pathological permeability to both the clotting cascade biomolecules as well as the whole gamut of lipoproteins. This deposition of foreign matter is understood for over five decades as being the causal moment of atherosclerosis, but it is still not widely accepted in 2015 that the collagenous and protein barrier of the artery built by vitamin C dependent enzymes is important to prevent this permeability event.
Some factions claim that loss of arterial collagen is causal to atherosclerosis without being very specific about the mechanism (where? the adventitia? the endothelial basement? The media? how? immune side? smc autophagic? oxidative? proteolytic? autolysis?) and refer to studies done before regarding deranged hepatic metabolism of cholesterol during scurvy which causes a certain hyperlipidemia by bile metabolism deficiency and consequent lack of fecosteroid excretion. Others will look at ratios of Collagens I, III, IV, and even V in the atherosclerotic plaque and their ratios during atherosclerosis. However, the specific mechanism of collagen loss and atherosclerosis has never been scientifically described in a definitive study until this one. Through simple logic, (common sense), it follows that singular or combinatory losses of the other arterial collagen subtypes would provide the same result experimentally, either in vitro or in vivo.
The Maeda paper showing that scurvy causes Evans Blue extravasation and gross damage to the arterial wall did not describe any atheromas, hyperplasias, or plaques because the mice die from scurvy before they can incur cumulative atherosclerosis. They did prove that scurvy causes arterial degradation to the extent that lipoproteins and anything else can enter the artery that can't transgress a healthy, vitamin C (ascorbate) replete artery wall.
The implied connection between atherosclerosis and scurvy is collagen. While ascorbate isn't the only vitamin involved in collagen synthesis, it is the only one that when absent will prevent proper polymerization of hydroxyl residues. There is nothing to debate in this regard. No ascorbate = no assembled collagen. There may be pro-collagen formation and its strands, but they will never be assembled correctly into their "stronger than steel" fibers without vitamin C, but remain a useless stockpile of components.
It is important to note that the correct ratios of the various collagens is exceedingly important. While much focus has been made on COL4 basement membranes in conferring tensile strength and resistance to metastasis, too much of COL4 without the other collagens in balance can cause mitochondrial death by integrin signaling abnormalities, as well as aberrant vitamin A processing. It is not as simple as to say "the more collagen the better." Not whatsoever is it that simple, and such a conclusion could be disastrous in clinic. Fibrosis is a disorder of too much of the wrong collagen in the wrong place at the wrong time and is a devastating disorder.
However, if the intrinsic collagens in the artery, such as COLXVIII, vanish, arteries become much more prone to lipid intrusion and the chain of events that occur after that. As such, the normal constituency of arterial collagens, many of them not even recognized by conventional histopathology stains and immunohistochemistry, prevent large particle lipoprotein intrusion. Collagen XVIII is a subtype that is virtually ignored in cardiology, yet possibly one of the most important subtypes. It logically follows that deficiencies in the most commonly acknowledged collagens of the arterial media and basement membrane, COLI, COLIII, and COLIV, would cause similar problems of pathological permeability to both the clotting cascade biomolecules as well as the whole gamut of lipoproteins. This deposition of foreign matter is understood for over five decades as being the causal moment of atherosclerosis, but it is still not widely accepted in 2015 that the collagenous and protein barrier of the artery built by vitamin C dependent enzymes is important to prevent this permeability event.
Subscribe to:
Comments (Atom)